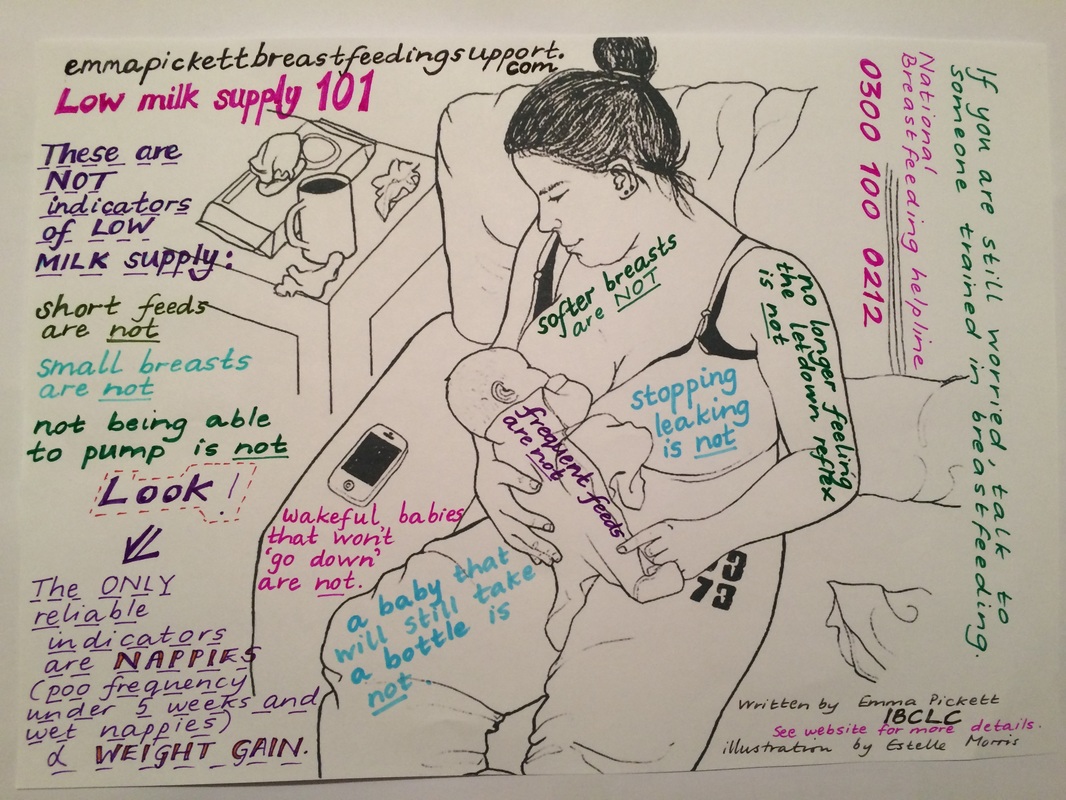

Image text by Emma Pickett, IBCLC. Drawn by Estelle Morris. Via emmapickettbreastfeedingsupport.com.
Everyone wonders. Many are convinced.
Around the time of milk regulation when the breasts feel like they’ve turned into empty pita pockets seemingly overnight, the world shudders with populations of postpartum nursing women who cry in atonement for whatever sin caused their sudden lactational failure.
But are you sure you REALLY have low supply?
Find out: “Perceived Insufficient Milk” by Diana Cassar-Uhl, MPH, IBCLC should be required reading for all first-time mothers.
If you have determined without a doubt that your supply is in fact low, you must find out why. Is it because you biologically cannot produce sufficient milk, or have you been booby-trapped? The former is incredibly rare (2% of all women), and the latter is unfortunately incredibly common in western society.
Or is there a problem with the baby that is keeping him from transferring enough milk? Have you recently introduced bottles, supplements, or pacifiers? Have you started a new medication or take up smoking again? Does your milk seem lower than usual because baby is at the precipice of a growth spurt? Has your supply temporarily dropped because you’re menstruating?
(Read the links in the Resources section below for even more real vs. commonly mistaken reasons for a decreased supply).
Supply & Demand…& Pumping
Brush up on your body’s process of establishing milk here. (Also note: the amount of milk you produce with a pump is NO indication of how much milk you are producing or can produce).
Breastfeeding works by letting down the milk when oxytocin has been evoked by the smell, sight, sound, touch, or thoughts of your baby. It’s pretty effective, to say the least. A pump, on the other hand, is nothing more than plastic machinery designed to literally pump the goods out of you, whether you like it or not (if your body doesn’t like it so much, it won’t respond so enthusiastically).
Your body is designed to feed your baby, not your pump, and it can only be tricked so much. If your breasts only come up with an ounce of milk after an hour of pumping, understand that your baby would receive exactly what s/he needs if effectively nursing for the same amount of time — likely much more than an ounce.
Likewise, the amount a baby drinks from a bottle is not a clue as to how much she takes from the breast, or should take from it (they tend to drink more quickly and focused on quantity from a bottle because the flow is not entirely self-paced).
Signs That Baby is Getting Enough Milk
It can be difficult to trust your body and your baby to play nice enough together that you needn’t worry — especially in our modern culture wherein everything is measurable, containable, with explicit applications and directions. There’s no gauge on your bra falling and rising as the tanks empty and refill. But you can still be sure baby is getting what s/he needs without trying to figure out how to get a measuring spoon in your boob.
Pay attention to these:
- Track dirty diapers.
Younger exclusively breastfed babies have loose, frequent stools (which many people still mistake for diarrhea because they’re accustomed to comparing against the more solid, constipated poo of formula-fed babies). Some exclusively breastfed babies older than six weeks can go one-two weeks without a bowel movement and be perfectly healthy. If stools remain loose and/or curdy, constipation isn’t a concern. Remember that breast milk is super digestible and bio-available, which means the baby actually uses a large portion of it and leaves less as waste product than formula. Click here to learn about normal/abnormal newborn baby poops and the, uh, colorful metamorphosis that occurs as baby ages.
Dr. Sears says:
“While urine output tells you that baby is getting a sufficient quantity of fluid in the milk, stool output tells you about the quality of the milk, (i.e., whether baby is nursing long enough and well enough to trigger mother’s milk ejection reflex, which brings the creamier, high-calorie hindmilk).”
- Track wet diapers.
What’s even more important than scrutinizing poo is tallying up wet diapers. This might get a bit tricky if you’re practicing elimination communication or going the diaper-free baby route, so let’s put it this way: a young baby should urinate at least six times in a 24 hour period (for a baby older than four days, or after the mother’s mature milk has come in). Put 2 tablespoons of water in a dry diaper to help you visualize what ‘one’ wet diaper looks/feels like for a baby less than a month old, and 4-6 tablespoons for older babies (note the difference between disposables and cloth if you use both). Your baby’s pee should be light in color; dark honey color can signal dehydration.
- Track feedings.
Counting breastfeeding sessions can get confusing (you might wonder, does only one side count as a full feeding? Does a five minute feeding count? Does a lot of spit-up negate the feeding?) but don’t bother getting too scientific about it. Feed on cue and offer in between; you’ll learn pretty quickly what counts as a full feeding session for your own baby, and can meet the necessary 8-12 minimum feedings per day.
- Allow your baby to pace the feeding.
Don’t rush him to finish up after a proscribed amount of time. Sometimes babies will suck efficiently and purposefully enough to draw out what they need in five minutes, and other times they will linger on the breast for an hour. Remember, they are following their instinctual bodily cues for satiety — they are wired to do what they need to ‘get enough,’ so let them try.
- Learn about normal weight gain in an exclusively breastfed baby.
In the first days of life, most babies lose a small percentage of their birth weight and this is normal. After baby has regained these lost ounces, baby should ideally gain 4-7 ounces per week (measured from the baby’s lowest weight after birth, not the birth weight). Some babies don’t return to their birth weight for several weeks, though. If that’s the case and s/he appears otherwise perfectly healthy, have a lactation consultant and your pediatrician assess and monitor (using WHO growth chart standards) to make sure baby doesn’t have an underlying medical issue (don’t rush to blame your milk!). Don’t forget that increasing head circumference and length/height are valuable markers for growth, too. Read more to find out if your baby is gaining enough weight in my post here.
Slow Letdown
A lazy letdown can be, well, a damn letdown.
Baby’s like, “What you waitin’ for, Ma? Christmas?! Let’s get this milk show on the road!” and you’re just sitting there like, “Okay, so you mean… I’ve been scrunched up in this poorly-postured nursing position for ten minutes already and you haven’t even started drinking yet??” …. “F%@&#!!”
Before resorting to ripping out your hair (if postpartum shedding left you with any, that is — ha), let’s discuss causes and solutions. Click here for your guide to the common causes of a slow letdown reflex.
Sorry, you can’t blame your baby for this one: Dr. Jack Newman says, “Incidentally babies are not lazy, they respond to milk flow.”
So get your milk flowing more quickly with breast compressions. Definitely try this BEFORE resorting to the following galactogogues (as always, consult a doctor first before turning yourself into an herbal science project).
- Mother’s Milk Tea (click here for possible side effects).
- Fennel might help, but use caution.
- The ever-popular Fenugreek can help, but some women should avoid it.
- Rescue Remedy can ease anxiety and tension that may be stifling your letdown reflex.
- Other last resort measures include Ignatia 6x and domperidone. Safety and risks of these drugs should be discussed thoroughly with your doctor before use.
- Research the risks of Reglan.
Resources
- “How can I tell if my baby is getting enough milk?” – LLLI
- “Increasing Low Milk Supply” – Kelly Bonyata, BS, IBCLC
- “Losing Your Milk: What seems like dwindling milk can actually be normal changes in baby and you” – Teresa Pitman.
- Low Milk Supply: Information and Support for breastfeeding mothers
- Making More Milk (book) by Diana West, IBCLC, and Lisa Marasco, MA, IBCLC


I think it is also VERY important for nursing moms to realize that what they pump is not a good indicator of their actual supply… So many doctors will have a mom pump to see how much milk they have in there and when only a drop or three comes out they are convinced they have a poor supply. Babies can nurse out way more than an old pump any old day… It’s a fact.