
Here are twelve questions we don’t often think to ask about circumcision.
1). What kind of training does a person need to be able to perform a circumcision?
Short answer: None.
Longer answer per this PubMed survey published in Pediatrics:
“Residency training standards are not consistent for pediatric, family practice, and obstetrical residents with regard to neonatal circumcision or instruction in analgesia/anesthesia for the procedure.
Training with regard to pain relief is clearly inadequate for what remains a common surgical procedure in the United States. Given the overwhelming evidence that neonatal circumcision is painful and the existence of safe and effective anesthesia/analgesia methods, residency training in neonatal circumcision should include instruction in pain relief techniques.”
“Conclusions: Our survey findings indicate that most physicians performing neonatal circumcisions in our community have received informal and unstructured training. This lack of formal instruction may explain the complications and unsatisfactory results witnessed in our pediatric urology practice.
Many practitioners are not aware of the contraindications to neonatal circumcision and most non-surgeons perform the procedure without being able to handle common post-surgical complications.“

2). Who is the person performing the surgery?
Technically, anyone is legally able to perform a circumcision. However, according to this article published in Pediatric News, most ‘medical’ and religious circumcisions in the U.S. are performed by:
- An obstetrician (70%)
- A family physician (60%)
- A pediatrician (35%)
- A mohel (at home or a Jewish facility)
Surgical circumcision revisions are typically performed by a pediatric urologist. If need arises to address penile adhesions resultant of circumcision, they can be ripped apart manually at a regular pediatrician’s office (parents are instructed to continue this at home as necessary).

Via Intact Houston
3). How do they know how much skin to cut off?
They don’t “know” — it’s guesswork. There is no way to predict how much a newborn baby’s penis will grow and mature as he ages.
This is one reason (of many) why, if the owner of a body should choose himself, a circumcision performed as an adult is preferred and safer than undergoing surgery before complete sexual maturation. The penis has fully developed by adulthood, so the surgeon can ascertain without question not only how much foreskin should be removed to ensure sufficient shaft skin will remain, but can also preserve the ultra-sensitive frenulum (which is almost always destroyed or eradicated by neonatal circumcision).
Circumcision performed in a hospital is more likely than in other settings to remove all foreskin (in some cases some amount of shaft skin as well). Consequences of excising too much skin may later in life lead to painful erections, tight skin, chordee (bent penis), and hairy shaft.
Insufficient foreskin removal may beget skin bridges and adhesions, wherein the skin remnant reattaches to the glans, trying to cover it as nature intended. Because the normally united membranes have been forcibly broken apart, at this time skin connecting directly to the glans is dangerous. The adhesions must be regularly torn until they cease attempts to reattach.
Per a Scientific World Journal article, complications from the Gomco method of circumcision:
“It is important to assure that the metal bell completely covers the glans, otherwise insufficient skin will be removed and accidental incision into the glans is possible. A bell which is too large will result in removal of too much skin. As mentioned, overly aggressive retraction of the skin through the platform can lead to excessive skin removal and subsequent corrective surgery; conversely, insufficient drawing up of the skin will lead to an incomplete circumcision, which may also require corrective surgery.”
Complications from the Mogen method of circumcision:
“The possible complications include insufficient or excessive skin removal or asymmetric redundancy and glans amputation all due to improper clamp placement.”
And the Plastibell:
“The associated complications include incomplete circumcision due to inadequate bell placement or slippage of the Plastibell while tying the hemostatic suture, and glans injury or bleeding due to inadequate hemostatic suture placement.”
“Wound dehiscence and degloving injuries of the shaft are possible following using any of the techniques described above for neonatal circumcision. De-gloving injuries result from excess skin being drawn up into the clamp and then amputated.
While, less likely, improper determination of the amount of skin to remove during free-hand circumcision may occur.“

Via Intact Houston
4). If American medical practitioners continue to routinely recommend and perform this surgery, despite current knowledge of its harms — can we trust them to teach proper care of an intact penis?
In a word, no. Given the poor track record of Western medical practitioners tasked with assessing normal male genitalia, parents of intact boys must always assume their ignorance (and that of babysitters, daycare workers, relatives, other caregivers) of what proper care entails.
This article does a wonderful job explaining why many American doctors remain largely confused:
“First, if we look at the AAP (American Academy of Pediatrics) recommendations, it wasn’t until the 1990s that the AAP finally warned against the harms of forcible retraction and outlined the development of the foreskin in the intact boy. [Before] it was widely believed that parents needed to retract their intact sons for ‘cleaning’. [T]his lead to many complications for intact boys and resulted in many otherwise unnecessary circumcisions.
Second, there was a preliminary study of about 300 boys to determine the average age of the development of a retractable foreskin [which] concluded that most boys will become retractable by age three. This out-dated study set an expiration date in the minds of the medical professionals. A follow up study of thousands of boys concluded that, in fact, only 50% of boys are retractable by age ten. Many doctors, unaware of the most recent study, still operate under the misinformation of the preliminary study.
Third, the development of the prepuce is not taught in medical schools. There is no discussion of how the prepuce is structured, how it changes throughout childhood and its protective and sensory functions. Essentially, the only thing medical students learn is how to amputate the foreskin. Some medical students may learn about the condition of phimosis but they are not informed that this only applies to adult men, as children’s foreskins are designed to be tight.“

Via Intact Austin
It’s not terribly difficult to keep a biologically normal penis clean and healthy. People have managed this since the dawn of mankind, and other animals have successfully survived the care-taking of their foreskin since the advent of their own species, too.

Via Intact Houston
Someone please tell this lady?

Via Intact Pennsylvania
More resources:
5). Where does the money paid for a circumcision go?
According to Circumstitions, the direct fee for circumcision is but a fraction of the total cost (not including the bodily cost to the man whose foreskin was stolen).
Important to remember:
“Facility fees: The baby is usually already in a hospital, and the facility fees are not counted separately. In 1990-1, Mansfield et al. calculated that a baby and his mother spend an extra 0.26 of a day in hospital if he is circumcised. Generalizing the difference in hospital length of stay to the United States suggested an annual cost then of between $234 million and $527 million beyond charges for the procedure itself.
We can get another estimate of the cost from the fees for outpatient circumcision, in South Carolina $570, in Minnesota $288 – $800.
Anaesthesia: Louisiana spent $121,695 on circumcision anaesthesia in 1999. (There were 10,763 circumcisions, but a significant proportion would have been committed without anaesthetic.) Other figures are unobtainable.
Supplies: Sterilized instruments, Circumstraints(TM), clamps and/or Plastibells(TM), antiseptics, syringes, gauze pads, etc.
Another estimate of the total immediate cost is as much as $2000-2500 for every male born (around 50.1% of all births in the US), based on the multiple added costs for each delivery which ends in a circumcision adding up to around an extra $2000-2500. The extra charges were around $1000 in 1991.”
A circumcision in the U.S. can cost between $300 – $3,000. Revision or corrective surgeries can cost hundreds or thousands more.
Dollars & Sense: The Business of Circumcision wrote:
“If a doctor circumcised just five boys each week at [the average] rate, they can pull in $176,208.20 annually, and that is if they take two weeks vacation!
To put that in perspective, that is about 25 minutes of work per week (as opposed to the 2400 minutes per week the rest of us work), for which the doctor and/or hospital are paid over 4 times the national average wage index for 2009.”
As you can see, this guy gets a big cut for making the cut. 
6). What happens to amputated foreskin, and who profits from its sale?
Since the 1980s, private hospitals have been caught romping in the business bed with private bio-research laboratories and pharmaceutical companies that seek their patients’ castaway foreskin for research purposes.
Foreskin (also listed as “neonatal fibroblast cells”) are stolen from unconsenting babies and used for/in:
- Skin grafts and transplants (Apligraf, AlloDerm, and TransCyte are three products)
- Cosmetic skin cream (as Nouricel, an ingredient made from harvested neonatal foreskin, in Oprah’s SkinMedica which can sell for $100 per bottle)*
- Dermagraft-TC (It sells for about $3,000 per square foot. One foreskin contains the genetic material to grow 250,000 square feet of skin).
- Fibroblast injections to compete with Botox (by the company Vavelta)
Who profits from neonatal circumcision?
- Performing doctors
- Makers of patented Plastibell and Circumstraint, who can charge what they want their surgical devices/apparatus (the Mogen company was recently sued out of business for its product’s role in an a shockingly high number of partial glans amputations)
- Biomedical companies to produce insulin
- Research companies for biomedical analysis
- Advanced Tissue Sciences (ATS), Organogenesis, BioSurface Technology, Genzyme, and Ortec International use foreskin cells to experiment in making artificial skin
- *Oprah
Is it ethical to steal an amputated body part from a person who does not give permission, is not informed about what happens to his body part, and will never see a cent of profit from its sale and use? The parents who consented for its removal aren’t privy to the future of their baby’s tissue either and many wrongly assume it is simply discarded along with the hospital trash.
“Parents should be wary of anyone who tries to retract their child’s foreskin, and especially wary of anyone who wants to cut it off. Human foreskins are in great demand for any number of commercial enterprises, and the marketing of purloined baby foreskins is a multimillion-dollar-a-year industry.” – Paul M. Fleiss, MD in Mothering Magazine, Winter 1997, pg. 39
Organogenesis, one company that profits off stolen newborn foreskin, dares to claim the cells in its product “are derived from donated infant foreskin.” Donated?! That never happened, foreskin reaper Organogenesis.
To be accepted as offerings to noble causes in the name of scientific progression, it seems more ethically sound that an amputated part is legally and willingly donated by an adult of his own body or perhaps the parents of a stillborn baby. This body part does not begin to ‘belong’ to other entities once separated from its original owner any more than a luxury robbed by a thief. Ownership by the cheat of force does not an ownership make.

More resources:
- Link to the website shown in the graphic above
- Neonatal Foreskin Epidermal Keratinocytes go for $250 at the Coriell Institute for Medical Research
- 1 mL of frozen neonatal foreskin goes for $599 on ATCC biological resource center
- Interest in circumcision more than foreskin deep
- Foreskins For Sale
- Stealing Foreskins: The Science of Skin Grafting
7). How much blood loss is needed for an infant to hemorrhage? Or to die?
Per Dr. Momma:
“A baby only needs to lose 1 ounce of blood to hemorrhage, and just 2.3 ounces to die as a result of this blood loss.
In their statement on the increased dangers of neonatal circumcision, Doctors Opposing Circumcision (DOC) physicians and surgeons reported:
…Infants have a miniscule amount of blood in their tiny bodies and can tolerate only about a 20 percent blood loss before hypovolemia, hypovolemic shock, and death.
A 4000 gram male newborn has only 11.5oz (340 ml) of total blood volume at birth, 85 ml per kilogram of weight. Blood loss of only 2.3oz, (68 ml), 20% of total blood volume at birth is sufficient to cause hypovolemia. Many newborns, and especially premature infants, weigh much less and a smaller amount of blood loss would be sufficient to trigger hypovolemic shock in those infants…
This is one reason that so many clamps are used on the amputation site when the prepuce organ is removed during circumcision surgery – to stop the ‘bleeders.’ It is also the reason these clamps are left in place at least 5 minutes after cutting is complete (as horrifically painful as this is for a newborn who cannot be put under general anesthesia at this stage in life).”

What 1 oz of blood (the amount needed for critical hemorrhage) looks like in a shot glass. Via DrMomma.org.
More resources:

Image by Anthony Webster
8). Why do experts in female anatomy typically perform Routine Infant Circumcision, which takes place on a specific part of male anatomy?
This is a good question that prompts one to consider the consequences of such incongruence of personal experience/acquired education with the practiced reality.
A Pediatrics Study found that obstetricians perform 70% of male circumcisions in the U.S.
Let’s define Obstetrician (noun) –
A physician or surgeon who specializes in women’s reproductive health.
And… male anatomy too… right??

9). Has the American Academy of Pediatrics (AAP) ever advocated for female circumcision?
As for the AAP, the answer is yes (surprised?).
On April 26th, 2010 (interestingly, the same day that legislation was passed to ban overseas transport of minors to carry out FGM in other countries, also called “Vacation Cutting”) they issued a statement that advocated for “federal and state laws [to] enable pediatricians to reach out to families by offering a ‘ritual nick’,” including pricking and minor incisions of girls’ clitorises.
A form of sexual violence once called “Female Genital Mutilation (FGM)” was then termed “Female Genital Cutting (FGC) or Ritual Genital Cutting.” How politically correct.
The AAP retracted their policy update within a few months of advocacy groups strongly protesting it.
This isn’t the first time female circumcision has been addressed in the U.S. In fact, a surprisingly rich history precedes its current state of practice here.
A Quick Timeline:
1888 – Dr. Harvey Kellogg (of Corn Flakes fame) encouraged genital cutting of both sexes and also wrote in his 1888 book Plain facts for young and old: Embracing the natural history of hygiene and organic life, p. 106-7:
“In females, the author has found the application of pure carbolic acid to the clitoris an excellent means of allaying the abnormal excitement, and preventing the recurrence of the practice in those whose will power has become so weakened that the patient is unable to exercise entire self-control.”
1960s – Female circumcision was endorsed by American medical journals through the 1960s for many of the same “benefits” supposedly also offered by male circumcision.
1970s – A 1973 cover of Playgirl Magazine cover advertised female circumcision as “The Kindest Cut of All.” The article is read here. Another article appeared in a 1975 issue of Playgirl, entitled “$100 Surgery for a Million-Dollar Sex Life.”

Via Peaceful Parenting/Dr. Momma
1997 – Female circumcision of minors was made illegal under U.S. federal law on March 30th, 1997, and 23 states now have laws against it.

Via Population Reference Bureau
Today – Many plastic surgeons and gynecologists routinely suggest and promote cosmetic genital cutting for women to improve ‘self-esteem’ and ‘aesthetic appeal.’
One such surgery is called labiaplasty (a trimming of the labia to be smaller and more symmetrical), a procedure the American Society of Aesthetic Plastic Surgery listed as one of the fastest growing cosmetic surgeries for women in the U.S.
The patients are of age to grant consent, but one cannot deny the role of “Designer Vagina” marketing in recent Western society, perhaps stemming from mainstream availability of modern pornography and images of modified vulvas; the popularization of Brazilian waxes; airbrushing; and hypersexualized, culturally-dependent ideals of the female body.
Notice that labiaplasty falls under Type II(a) on this chart of recognized forms of FGC/FGM and MGC/MGM. Reduction of the clitoral hood is another cosmetic surgery on the rise in the West, as well as vaginoplasty or “Vaginal Rejuvenation” (which often involves narrowing of the vaginal opening to improve tightness — sometimes for valid medical reasons but more often to regain what’s advertised as ‘youthful’ feel and appearance).
Where can you find these forms of genital cutting on the chart below?
Another question worth consideration: From where do you think the cosmetic reasoning for male circumcision derives?

Via DrMomma.org
10). Must fathers, sons, and brothers match? But really — must they?
It’s never too late to improve and rework our plans and perspectives, and we should do better when we know better. This is the best anyone can do.
Fathers, brothers, and sons don’t need to ‘match’ any more than mothers, sisters, and daughters do — in fact no matter what we do or have done in attempt to mold them into each other’s reflections, they’ll never match anyway!
If the father feels strongly about continuing a tradition of matching genitalia, make sure he understands the true meaning of ‘practice what you preach.’ Should he insist upon permanently altering his son’s body to ‘match,’ would he so easily agree to undergo surgery himself to achieve the same goal? Would he expect the mother of his daughter to do the same? Would he ever demand that his daughter do such a thing?
Here’s how a child in one family made sense of the ‘need to match’ argument:
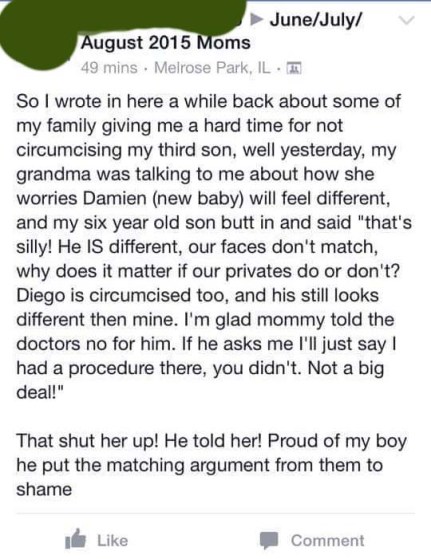
Via Facebook
11). If babies sleep through circumcision, why does the surgery board have restraints?
Because they don’t sleep through circumcision, and it would be impossible to perform a delicate, multi-step surgery on a baby struggling for his life.

Shared by Krista Johnson via Saving Our Sons Facebook page
Nurses admit they lie to parents after the surgery, because who wants to hear their baby screamed, choked, eliminated on themselves, strained, and vomited until they passed out?
“The ob nurse had quite a few things to say about hospital policy and what they are advised to tell parents after a circ. They are not allowed at any time to say ‘poor baby’ after a circ. Not in front of the dr’s or parents. They are not allowed to make the parents or dr’s feel responsible for the pain an infant male must endure.
They are told when they bring the baby back to his mother to say either ‘What a good baby. He didn’t make a peep.’ Or ‘What an angel. He slept the whole time. You have a very happy baby on your hands.’ They think this will make an uncomfortable situation better.
I asked if she has ever seen a baby actually sleep through a circ. She looked at me as though I was crazy. ‘Of course not.’ Have you ever seen a baby not cry at all? ‘No.’
…Sometimes at the first diaper change afterward the mothers are very distraught at what they see. It’s obvious it’s not a little snip… they’ll ask ‘Is it supposed to look like this?’ In which [case] she is to respond ‘Oh everything looks fine. It will heal up in a day or two.’ Even though she knows it is not fine.” – Circumstitions
Then of course, many babies undergoing circumcision fall into a state of psychological shock that may look quite a bit like ‘sleep.’ Other mammals who are skinned alive may hold an expression of similar resemblance — a solemn, zoned-out, detached look not to be mistaken with slumber.
This is shock, and it is not a peaceful state. It is an acute reaction to enormous stress endured in a situation of no escape. The victim remains conscious, but his emotional systems shut down in attempt to cope with the immensity of physical pain.

Via SavingSons.org
12). Is neonatal/child circumcision a form of sexual assault?
Circumcision performed on female minors has long been viewed by Western society as a form of sexual assault. When the same argument is made for male minors, a startling amount of confusion and pushback abounds, despite the clear gender discrimination playing out right under our noses.
Two United Nations reports (see: United Nations Document No S/1994/674) perceive sexual assault on males including circumcision as “torture and a violation of human rights.”
According to RAINN, sexual assault includes “penetration of the victim’s body” and “fondling or unwanted sexual touching.” Can this definition apply to the circumcising physicians’ act of manually stimulating a newborn boy’s penis to ensure he has an erection, making possible the process of then ripping, crushing, and severing it?
According to Wikipedia, rape is “a type of sexual assault usually involving sexual intercourse or other forms of sexual penetration perpetrated against a person without that person’s consent.” This includes forcible sexual penetration with an unknown object (includes any foreign object, substance, instrument, or device, or any part of the body).

Circumcision tools used during Gomco method cutting.

By Aubrey via Saving Our Sons Facebook page

Via Intact Houston
It is well-known that sexual assault and rape can trigger lasting emotional and mental harm in survivors. It is much lesser-known that a baby’s brain psychology is in fact permanently altered by circumcision surgery.
“[C]ircumcision affected most intensely the portions of the victim’s brain associated with reasoning, perception and emotions. Follow up tests on the infant one day, one week and one month after the surgery indicated that the child’s brain never returned to its baseline configuration. In other words, the evidence generated by this research indicated that the brain of the circumcised infant was permanently changed by the surgery.” – Dr. Paul D. Tinari, Ph.D.
- List of studies: Babies remember circumcision pain (All U.S./Canadian studies on circumcision pain were halted early due to the high degree of infant trauma).

